Personalized Medicine – Myth, Pipe Dream or Realizable Promise?
This Blogpost was first published on the 4th of April, 2008.
Milestone: This blogpost and the author were referenced by the Partners Healthcare Center for Personalized Genetic Medicine in 2008 , the Center for Personalized Healthcare at the Ohio State University and quoted by the 2009 Personalized Medicine Conference at the Harvard Medical School.
Personalized medicine in recent times, has attracted significant hype as well as pessimism from a number of quarters including the Pharma industry that has often perceived this as “avant garde†and a grandiose vision that is way out there and not yet ready for useful value delivery to real-world patients and consumers.
So it was with a mixture of curiosity laced with healthy doses of pessimism that I attended the Personalized Medicine: A Call to Action Conference, November 29th and 30th, 2007, at the Harvard Medical School. The Conference was orchestrated by Dr. Raju Kucherlapati, Scientific Director of the Harvard-Partners Center of Genetics and Genomics and Paul C. Cabot Professor of Genetics at the Harvard Medical School, a pioneer and thought leader in the Personalized Medicine arena, in close collaboration with the Personalized Medicine Coalition (PMC) led by Dr. Edward Abrahams.
I must say I was pleasantly surprised by the august assemblage of stake holders from academia, large and incipient producers (pharma, bio-tech, diagnostics, medical devices), healthcare providers (physicians and hospitals), payers, as well as regulators. Michael Leavitt, secretary of Health and Human Services (HHS) delivered the opening, inspiring keynote address clearly signaling that Personalized Medicine (P/M) is a significant agenda issue and one whose time has come(1).
 Equally encouraging was the keynote presentation by Kathleen Behrens, member of the President’s Council of Advisors on Science and Technology (PCAST) highlighting the progress made by this body on studying the relevant facets of Personalized Medicine, to craft their recommendations for the president in their report that is due in 2008. Their comprehensive recommendations will highlight pragmatic yet far reaching policy changes that will need to be implemented to overhaul the ailing US Healthcare system and bring P/M to fruition.
What is Personalized Medicine? Why is this significant for Patients and Healthcare?
“Personalized Medicine means knowing what works, knowing why it works, knowing who it works for and applying the knowledge for patientsâ€, is perhaps the most succinct articulation of P/M from the honorable Mr. Michael Leavitt, secretary of Health and Human Services (HHS). This implies delivering treatment to patients that is proactive, predictive, personalized and participatory unlike the status quo today.
By way of the “trial and error†medicine (also sometimes referred to as “intuitive medicineâ€) practiced across the world today, the doctor makes a “most likely†diagnosis consistent with symptoms and them prescribes what he/she considers appropriate treatment comprising drugs, devices or surgery. If the treatment does not work and presents significant side effects or adverse events, the doctor most likely would alter dosage or prescribe an alternative medicine. This iterative cycle is repeated, until the diagnosis and treatment that actually presents the desired clinical outcome in the patient is reached. The paradigm has reached a point of diminishing returns as evidenced by the fact that most drugs prescribed in the U.S. today are effective in fewer than 60% of treated patients(2)!
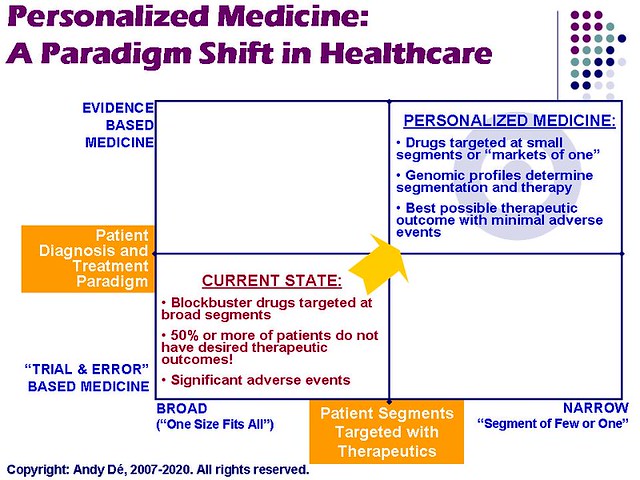
Personalized Medicine, au contraire, uses far more sophisticated and refined diagnostic testing to arrive at the precise diagnosis aligned with the person’s genetic makeup at the molucular level, and hence is also often referred to as “evidence-based medicine†or “precise medicineâ€. P/M would first map a person’s genomic profile and then ensure mapping of this profile to the treatment to maximize efficacy and the best therapeutic outcome (often with life and death implications), while minimizing adverse events (please see the framework below). The closest real-world analogy to P/M is the recruitment process that matches a person’s job to his/her education, experience and skill sets as laid out in his/her profile (resume) to ensure the best fit for the job, or the “nirvana notion†of targeted marketing to “markets of oneâ€. P/M is in essence, delivering “mass customization†to people in a healthcare context at an affordable cost.
Â
Let’s consider what is perhaps the best known example of how P/M can actually save lives in the real world.
Herceptin, a monoclonal antibody delivered by Genentech (often recognized as the pioneer of the bio-tech industry), has been found to be particularly efficacious as a first line treatment with chemotherapy, in treating aggressive forms of breast cancer in women whose tumors have an overabundance of HER 2, a protein that promotes cell growth. Herceptin has been found to reduce the likelihood of cancer spreading to other parts of the body in these patients by a remarkable 53% compared with traditional chemo therapy alone, according to a 2005 study. This is also compelling from a cost-benefit perspective. The tests to detect whether a breast cancer patient has an overabundance of HER 2 protein (and thereby a candidate for Herceptin) costs a mere $ 400 and potentially saves thousands of dollars by preventing the cancer in HER2 patients from spreading to other parts of the body and by not treating HER 2 negative patients with a drug that won’t help them (2).Â
Â
 A very similar business case (4) also presents itself for patients with high cholesterol who are prescribed high statins for treatment – these tend to be ineffective or not completely ineffective in a significant number of these patients!
 Â
What are the Key Barriers to realizing Personalized Medicine (P/M)? Â
The conference (1) identified six challenges that need to be collaboratively addressed to bring P/M mainstream:
1. Reimbursement – Who will pay for the incremental cost of delivering P/M? This is perhaps the most significant barrier given the already high cost of delivering healthcare today,that is growing at 10-13% annually and consumes almost a fifth of the US GDP today. According to Michael Leavitt, payment systems today are “fundamentally flawed and reward providers and physicians for volumes and not value deliveredâ€. As well, health Insurance needs to be dramatically improved to assure affordable health insurance for every American. Besides, why should payers pay for P/M without clear, compelling and unequivocal demonstration and evidence of superior therapeutic outcomes in patients that can be delivered cost effectively?
2. Business Models – What are the new business models that companies need to enable to render P/M a reality? The Pharma industry is largely driven by the Blockbuster model (please see my earlier blogpost “Branded Pharma – Who moved my Blockbuster Cheese?!â€) that is being severely constrained today, with a huge fall in innovation productivity for most Pharma companies – a mere 22 NMEs (new molecular entities) have been approved by the FDA in 2007 against 80+ NMEs in 2000. Given this constrained innovation pipeline, what will viable business models that will ensure delivery of “targeted therapeutics†to very small patient populations for superior outcomes, while assuring profitability for Pharma/Devices/Diagnostics companies look like?
3. Connectivity and lack of Business Process Integration – Given the archaic paper based processes, what is the IT infrastructure needed to integrate the Healthcare Value Chain into a coherent system that will enable P/M? Speaker after speaker at the conference pointed out the travesty of calling Healthcare a “system†given the lack of basic connectivity within the Hospitals and across the Healthcare value chain that presents really daunting challenges. These include facilitating collaboration among researchers, clinicians and the Healthcare Value Chain at large, accessing, processing and integrating clinical, genetic and genomic data from multiple, often heterogenous and disconnected sources, and having the robust IT platforms (software and hardware) built on common industry standards to do so.
4. Regulations – How soon can a new innovation be delivered while assuring safety, quality and efficacy? Current regulations and the three tier approval process significantly drive up the cost of delivering drugs to market ($ 800 MM – $ 2 Bn per molecule) with times-to-market of 7-10 years which does not lend itself to driving the agility that is imperative for P/M to become main stream. A radical redesign of the drug approval process is imperative for P/M to come to fruition.
5. Trust, Transparency and Confidence – What will it take for patients to see the clear and compelling value of P/M to enable large scale adoption? Patients today are extremely skeptical of the Healthcare and Life Sciences industries’ capabilities of delivering treatment at an affordable cost. Given the need to compile genomic profiles for each patient (priced at around $ 350,000 per profile today) at a reasonable cost while ensuring privacy, security and (laws to guarantee) non-discrimination further exacerbates these concerns.
6. Physician Behavior – How can the current mindset and practices of physicians rooted in “Trial and Error†medicine be changed across North-America and the Globe? Educating the thousands of physicians in North-America and across the globe (trained in the current paradigm) presents a daunting challenge with enormous cost and change management implications.
Â
How can these Challenges to Personalized Medicine (P/M) be overcome in the foreseeable future?
While the conference attempted to address each of the six issues identified above, potential solutions in three areas (reimbursement, business models, IT infrastructure) were deemed the most important, tactically addressable and are summarized below:
1. Reimbursement – Who will pay for Personalized Medicine (P/M)? The Payer Perspective
A number of large insurance companies as well as government officials articulated the need to support and enable P/M for the foreseeable future, which was extremely encouraging.Partners Healthcare initiative on P/M to unequivocally demonstrate this value i.e. superior therapeutic outcomes at a lower total cost while minimizing possible adverse events.
Cost containment (“potential savings from higher efficienciesâ€) is a high priority hot button issue for Congress (given that the government is the largest payer), especially in the light of the highest cost of healthcare in the world in the US. This is becoming a critical, “Big Picture†issue for the budget, finance and health committees in Congress, especially since rising Healthcare costs is compromising spend in other critical areas.
Comparing effectiveness of various treatment programs, services and products (including “Value-based Insurance Designâ€) is already being contemplated in Congress, as a first step to enabling metrics driven quality and performance improvements in Healthcare. Also significant is the awareness on enabling “holistic longitudinal accounting†i.e. increase spend upstream on accurate diagnosis to drive down costs downstream (treatment).
For insurance companies, having clear and compelling clinical evidence of superior therapeutic outcomes from P/M with accompanying data on driving down the “total costs of treatment†is imperative to demonstrate the value of P/M and drive a business case for funding, going forward. They still have a long way to go and are looking at harbingers of P/M like the Harvard Medical School –
Given the fatal flaw in the current system that pays for volume rather than value, the ability to measure (transparency) quality of delivered healthcare, comparable pricing for similar buckets of care and properly aligned incentives across multiple stakeholders, to deliver higher quality at lower costs are significant issues that need to be addressed for this to happen according to Michael Leavitt, the secretary of HHS. Policy amendments to effect these fundamental changes to healthcare reimbursement is currently being contemplated.
It was also startling to hear that 5% of all American patients (usually indigent and multi-morbid patients who use the emergency rooms as their mode of treatment in the absence of health insurance coverage) consume 95% of all healthcare costs! While bringing the 50 MM Americans currently without any health insurance into the healthcare system was a high priority for the government, it was also suggested that the most fungible way to design benefits enabling patients to choose the level of payments by “owning their own healthcare†and eliminating unnecessary and excessive spending while empowering them to make the best choices for themselves.
2. Who will deliver Personalized Medicine (P/M) and what will that business model look like? How do Regulations need to change to make this happen? The Producer (Branded Pharma, Bio-Tech, Diagnostics) Perspective
Advances in science and technology presents real potential in rendering P/M ubiquitous in the foreseeable future. The sequencing of the human genome has helped scientists link an ever increasing number of diseases to specific genes. As well, scientists have been making great strides in mapping the molecular pathways by which a change or mutation in a gene actually manifests itself in a disease. These innovations have enabled Pharma and Diagnostic/Bio-Tech companies to develop effective diagnostic tools like biomarkers that can distinguish the subtypes of what had been considered a single disease, as well as chemical agents that target each of these subtypes. This culminates in the ability to manage many fatal cancers as chronic conditions by attacking them early, resulting in more lives saved (2).
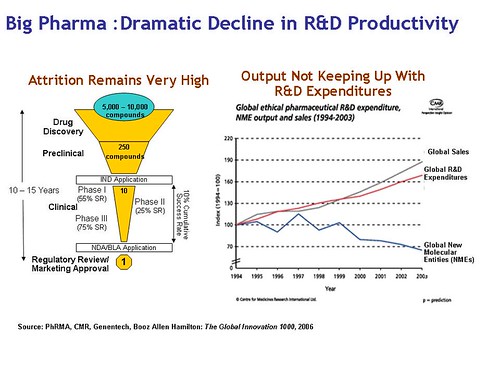
Critical to delivering P/M is a significant departure from the current Blockbuster Drug model by Pharma and life sciences companies. The economics of delivering a large number of molecules targeted at smaller patient populations will demand a radical transformation from the current model predicated on the discovery, development and commercialization of a very small number of molecules targeted at large patient segments. Given the dramatically declining productivity of current product pipelines (see figure below) in the large Pharma majors as well the potential loss of $ 160 Bn in revenues from expiry of current patents by 2015 (I have highlighted earlier in my blog posts “The 3 Questions that keep Big Pharma CEOs awake at night†and “Branded Pharma – Who moved my Blockbuster Cheese?!â€) and the demand by patients and providers for better clinical outcomes at a more affordable cost, Pharma companies may have little choice save embracing the radical transformation demanded.
The biggest challenge, according to the Pharma companies, is the science of drug discovery – how to identify and validate a genetic association with a disorder and then develop a molecule to address this. Pharmacogenomics and related technologies have driven significant advances in this arena, but there is still a long way to go.
Presentations from Eli Lilly, Astra-Zeneca, Siemens Medical Systems (SMS) and Celera Genomics encouraging in that these companies are proactively moving forward to enable P/M and believe they can sustain and reinforce their competitive advantage by doing so.
- Tom Miller, Group VP of Siemens Medical Systems (SMS) emphatically declared that SMS was “betting the farm on P/M†and has invested over 10 Bn Euros in acquiring companies and capabilities for “accurately characterizing diseases†in advance. He also cited the lack of an educated patient population that is prepared to “buy the vision†as well as the absence of “holistic longitudinal accounting†(invest more upstream in accurately characterizing disease to save treatment costs downstream) as perhaps the single largest barrier to success. As well, given the promise and advances in molecular diagnostics, and newer technologies like Pharmacogenomics, Toxicogenomics, Biomarkers, Imaging and Bioinformatics, the time is ripe for pharma and diagnostic companies to collaborate and move P/M forward.
- Given that almost 50% of all patients fail to respond to a certain therapy or treatment, segmentation of patient populations in clinical trials with development of appropriate diagnostic tools (“biomarkersâ€) to identify the most suitable target population as well as those at risk of significant adverse events. “Tailored Therapeutics†leveraging Pharmacogenomics and Biomarkers, is Eli Lilly’s answer to P/M to deliver drugs targeted for specific patient populations, with optimum dosage, at the appropriate time for intervention, with information tools to accommodate patient diversity as well as as questions specific to buyers, payers, physicians and providers. Pharma companies like Pfizer and Lilly are increasingly seeking approval for companion diagnostics (e.g. biomarkers usually based on DNA testing) to filter out patients that are likely to have adverse reactions to new drugs – a need currently fulfilled by bio-tech companies that provide DNA testing and analysis on the data as services. Adequately validated biomarkers (including their use in clinical trials) are a prerequisite for P/M to be realized viably, along with reimbursements to incent innovation and acceleration.
- Eli Lilly also presented compelling quantitative data demonstrating a business case for developing targeted therapeutics. The Return-on-Investment (ROI) from the lower total cost of treatment resulting from the superior efficacy and clinical outcomes in a smaller targeted segment, appropriately pre-qualified using companion diagnostics (enabling higher revenues from higher consumption and faster uptake), as well as the significantly reduced cost of adverse events and liabilities was higher than that of targeting large patient populations, with 50 – 60% efficacy of treatment, with the additional liability imposed by adverse events.
- From a regulations perspective, these Pharma and Bio-Tech producers expressed the imperative for granting additional periods of exclusivity for innovations targeted at smaller targeted populations, similar to the 7 year exclusivity for Orphan Drugs and pediatric drugs. Without these additional periods of exclusivity, the current economics of drug development simply does not lend itself to rendering targeted therapeutics viable – they would go out of business. As well, the imperative for shorter development cycles and costs demanding a fundamental re-thinking of FDA regulations is warranted.
Â
3. How will Personalized Medicine be enabled from a Technology/ IT perspective?
It is astounding that in the 21st century, archaic, paper based medical records, the resulting inaccuracies and inability to access this information in life and death situations results in over 80,000 deaths annually in the US alone.“Demand-Side EHRs: Who will make it Win-Win for patients to adopt?â€)
According to Michael Leavitt, connectedness and uniformity of standards in US healthcare sector does not exist today, hence does not quality this as a “systemâ€. Lack of standards and best practices in gathering and storing genetic/genomic information into Electronic Health Records (EHRs) are not in place and are a prerequisite for wide spread adoption.
The adoption rates of (18-23%) for EHRs by physicians and an even far smaller (2- 4%) rate of Personal Health Records (PHR) adoption is a huge challenge as well as an impediment to P/M that needs to be addressed with urgency (please see my previous blogpost and analysis on EHR adoption,
Here are some of the IT solutions that were proposed, to enable the level of intra and inter enterprise connectivity across the Healthcare Value Chain, demanded by P/M:
- Pharma and bio-tech companies are “swimming in data” (per Dr. Nadine Cohen from Johnson and Johnson) – what is missing today are effective tools to analyze the data and deliver meaningful analysis that will help them commercialize drugs faster. Use of drug disease modeling and scenario simulation is an idea whose time has come, to drive decision making re: new as well as mature drugs. As well, lack of collaboration across functions and trading partners and little to no visibility into downstream demand and patient insights is costing the Life Sciences industry especially Big Pharma, billions of dollars in value leakage by way of excess inventory, stock outs with life and death implications. Also exacerbating this is little to late visibility into adverse events and complaints resulting in huge penalties that can be significantly alleviated with tools for analysis of post-marketing data to understand and proactively impact patients who show adverse reactions to new drugs.
- Empowering customers with the information and decision support they need, to result in the best possible outcomes at the lowest cost, is the key. Using Microsoft Health Vault and similar personal health record (PHR) platforms are possibly the first step to enabling Personal Health Networks (PHNs) of patients with similar therapeutic issues – the wave of the future. This is fraught with significant challenges I have highlighted in my previous blogpost, “My PHR in Microsoft’s Health Vault: Confessions of an Early Adopterâ€. Evolution of the PHR from a passive data base of records to a decision support tool that will proactively help patients make the right clinical choices, lower information search costs and enable better collaboration with their physicians and care givers is a compelling vision for the future that I have persevered to elucidate in my previous blogpost, “Demand-Side EHRs: Who will make it Win-Win for Patients to adopt?â€
- The use of a robust computational platform as well as sophisticated predictive analytics similar to what other industries have already accomplished, is now long overdue in Healthcare to drive P/M. Bio-cities in Asia and the Middle East are developing comprising research, clinical and healthcare delivery within the context of one village or community that can deliver targeted treatment to patients.
- Enabling standards based interoperability, integration and exchange of data from EHRs (supply-side) and PHRs (demand-side), rules based decision support, as well as presenting them in a role-based context (what the physician demands vs. the patient needs) is a daunting challenge today. For instance, wouldn’t it be incredible if we could aggregate clinical and genomic data in the EHR, analyze this retroactively, to run in-silico clinical trials that will show physicians potential adverse events that may happen?
- Partners Healthcare in collaboration with Harvard Medical School has developed one of the first laboratories for P/M in this country within the healthcare system, harnessing genetics and genomics based data in the EHRs to drive decision support for real world patients. Some of the technical accomplishments at this initiative (3) are:
- Structuring and digitizing genetic and genomic information and incorporation within EHRs
* Creating applications to support genetic discovery and research
* Identifying computational, storage and software requirements and building the right IT infrastructure supports the P/M vision at Partners Healthcare to: Improve the quality and efficiency of research and clinical operations to positively impact and lower costs of delivering quality healthcare
– Integrate genetic test results into EMRs and EHRs
– Ensure the data integrity of the P/M business processes and workflows
Â
This is a significant milestone and a harbinger to realizing P/M. The Harvard Medical School -Partners Healthcare Center for Genetics and Genomics is also driving significant thought leadership by documenting and providing the IT requirements, architecture and applications for enabling P/M, to the department of Health and Human Services (HHS). This is a significant accomplishment that can potentially help establish the standards and best practices needed to proliferate P/M across the US using a networked model.Dr. Clayton Christensen, Robert and Jane Cizik Professor of Business Administration at the Harvard Business School (HBS) and author of the seminal and immensely successful works on business strategy- The Innovators Dilemma, The Innovator’s Solution and the just released Seeing What’s Next.
Can Personalized Medicine (P/M) potentially disrupt the current US Healthcare Model?
Â
Perhaps the most provocative perspective on P/M was presented by
According to Dr. Christensen, the ability of innovators to provide new products almost always outstrips the ability of most customers to adopt and utilize these innovations. Some of these are incremental while others are “disruptive†and have significant cannibalization impact on the incumbent technologies, with entrants nearly always winning! Disruption is facilitated when historically valuable and expensive expertise becomes commoditized thru scientific and technological advancements. Disruptive technologies deliver simpler, affordable, easer-to-use solutions at a lower cost of adoption for the customer. Combining disruptive technology with an appropriate business model is the recipe for assuring success
Applying his model of disruptive innovation to P/M in a healthcare context, Dr. Christensen prognosized the following:
- Molecular diagnostics and Interventional Radiology may be the “disruptive technological enablers†(“Precision Medicine†vs. “Intuitive Medicineâ€) of Healthcare that can potentially deliver simpler, most cost effective solutions with higher efficacy and safety for complicated diseases for patients.
- Therapeutics is where the money is made today but Diagnostics (coupled with Therapeutics) is potentially where money will be made in the Healthcare Value Chain, going forward. The analogy he provided was the shift in power in the PC industry from IBM to Microsoft and INTEL.
He however conceded that disruptive change in a Healthcare context is far more difficult given the power of the Payers and Regulators (unlike any other industry) to inhibit and constrain innovation. However, his presentation delivered some fascinating insights for the audience to ponder upon.
Key Takeaways from the Personalized Medicine Conference
 The Personalized Medicine: A Call to Action Conference was a seminal event that presented a realistic perspective and overview on the promise, the challenges, as well as the pioneering work being done to usher in the era of P/M, thanks to the thought leadership of Dr. Raju Kucherlapati, Scientific Director of the Harvard-Partners Center of Genetics and Genomics and Paul C. Cabot Professor of Genetics at the Harvard Medical School and his team and the Personalized Medicine Coalition (PMC).
Here is a concise summary of the key takeaways from this conference discussed in detail above:
- “The Future of Personalized Medicine (P/M) is now” and needs to be collaboratively driven by all stakeholders: academia, government, payers, producers, providers and physicians to bring P/M to fruition and deliver value to patients.
- Personalized Medicine is a significant line item in the current US government’s Healthcare agenda with a report and pragmatic recommendations for rendering P/M a reality to be presented to the President by his Council of Advisors on Science and Technology (PCAST).
- Current payment systems are fundamentally flawed – payments for volumes and not value. Insurance needs to be dramatically improved to assure affordable health insurance for every American. Holistic longitudinal accounting is a paradigm shift that is needed to enable appropriate reimbursement for P/M.
- Fundamental rethinking of the regulatory regime to assure safety and efficacy is needed to drive the agility needed. As well, additional periods of exclusivity may be imperative for targeted therapeutics to be rendered viable.
- Science and technology are both constraints for Pharma, Bio-Tech and Diagnostic companies to truly enable P/M as are the current economics of drug discovery and development. However, P/M is the way forward given the 50% efficacy of most treatments and therapies as well as the high incidence and cost of adverse events.
- Connectedness and uniformity of standards in US healthcare sector does not exist today, hence does not quality this as a “systemâ€. As well, this imposes huge inefficiencies and costs that are not sustainable, going forward. Transition to an electronic medical record (EMR)/electronic health record (EHR) system is imperative and will be driven by regulations.
- Lack of standards and best practices in gathering and storing genetic information into Electronic Health Records (EHRs) is a serious impediment, as is the abysmally low adoption of both EHRs and Personal Health Records (PHRs) by hospitals and patients respectively. The EHR is the cornerstone for connectivity to drive a 360 degree view of the patient as a first step to delivering value based treatment and superior therapeutic outcomes at the lowest cost.
- Trust, transparency, confidence, protection of the patient’s privacy and non-discrimination laws need to be in place for Personalized Medicine to become a reality. Consumer activism will happen once patients see value delivered from Personalized Medicine.
- Partners Healthcare in collaboration with Harvard University has developed one of the first laboratories for P/M in this country, within its healthcare system, harnessing genetics and genomics based data in the EHRs to drive decision support for real world patients. The ability of this initiative to clearly demonstrate benefits in the form of superior therapeutic outcomes and minimal adverse events at a lower total cost of treatment will be key to drive a business case for large scale adoption of P/M.
- P/M with its associated advancements and technologies can potentially disrupt the current Healthcare model in the US and lead to new classes of service providers delivery quality healthcare to the masses at lower costs.
Personalized Medicine (P/M) despite daunting challenges, presents enormous promise in terms of not only enhancing the quality of healthcare for patients i.e. each and every one of us, but also lowering the total-cost-of-healthcare.
Pioneering efforts like the Harvard Medical Partners Healthcare P/M initiative currently underway, the current portfolio of products already developed or under development, as well as the clear yet pragmatic commitments to P/M from all stakeholders involved i.e. academia, the government, the payers, the producers, the providers and the physicians was truly encouraging and inspires me to believe that P/M is no longer a myth, nor a pipedream and while not imminent reality, definitely a realizable promise that will positively and significantly impact the quality of our lives, in the foreseeable future.
 As always, your comments and feedback are welcome.
REFERENCES:
1. Presentations and panel discussions at the Personalized Medicine: A Call to Action Conference, Harvard Medical School, November 29th and 30th, 2007
2. Realizing the Promise of Personalized Medicine, Mara G. Aspinall and Richard G. Hammermesh, Harvard Business Review (HBR), pp 109-117, October 2007
3. Collaborating to Create Personalized Medicine, Business Case Study on the Harvard Medical School-Partners Healthcare Center of Genetics and Genomics (HPCGG), Hewlett Packard Company, 2007
4. The Case for Personalized Medicine, Personalized Medicine Coalition (PMC), November 2006.
 Go Home
Go Home
Commented on 7/18/2010
Very nicely written- explains the concept of Personalized Medicine in business terms for people who may not have a background in medicine or science. Good job, keep writing!
John Schesinger