The Personal Health Record (PHR): Who will make this “Win-Win” for Patients to adopt?
This blogpost was first published on September 27th, 2007.
Milestone: This blogpost was referenced and the author quoted by the Washington Post in an article entitled, ‘New Ways to Manage Health Data’, March 2008.

In my previous blogpost (“Can Life Sciences and Healthcare enable my evolution from “Passive Patient†to “Enlightened Prosumerâ€?), I have articulated my vision for the Electronic Health Record (EHR) and the incumbent benefits that would potentially enhance both quality and span of life, predicated on a paradigm shift – proactive, intervention based healthcare that would be far more cost-effective to deliver and yet assure timely and superior therapeutic outcomes.
In this context Microsoft’s announcement of its PHR Platform, the Health Vault, for Personal Health Records (PHR) under Peter Neupert’s leadership, and the support of Microsoft’s leader Steve Ballmer and its visionary founder and philanthropist par-excellence, is indeed encouraging. Particularly compelling is the support from partner organizations like the American Heart Association, Johnson & Johnson LifeScan, New York-Presbyterian Hospital, the Mayo Clinic and MedStar Health, a network of seven hospitals in the Baltimore-Washington region, that augurs well for Microsoft, given their success in driving alliance enabled solutions into the marketplace. Given Revolution Health’s (founded by Steve Case) announcement of it’s EHR last year and potentially, a competing EHR solution from Google in the foreseeable future, large scale patient adoption of Personal Health Records (PHRs) from one of these vendors will be mission-critical for success.
As well, Healthcare Solution Providers like G E Healthcare (headed by Joe Hogan), Siemens Medical Solutions (headed by Janet Dillone), Cerner, Misys and Enterprise Software Providers like SAP, and many others also provide Electronic Health Records (EHRs)Â targeted at Physicians and Hospitals.
Any new solution for Healthcare needs to address the needs of the 5Ps – Patient, Physician, Payer, Producer and Politicians. Given President Bush’s mandate for EHR adoption across all US hospitals by 2010 (which addresses politicians, payers and producers), the single largest challenge for PHR adoption and ubiquity, is patient adoption on the demand side and to a lesser extent, the physician/nurses/hospital adoption on the supply side.
PHR adoption by Customers – Daunting Challenges
Key to enabling this adoption is an understanding of the issues and challenges that I have modeled on the framework below, adapted from a seminal article entitled, ’Eager Buyers and Stony Sellers – Understanding the Psychology of New Product Adoption’ by John T. Gourville, Harvard Business Review (HBR), June 2006. The key premise is that the greater the level of change in customer behavior needed, the greater the barrier to customer adoption, despite the promise of value delivered by the new product. Gourville makes the point that producers of innovation often overestimate the customer adoption by a factor of 3X while consumers allocate significant value to their current product or service and demand a value proposition that is practically 9X times that offered (perceived) by their current product or service.
This framework enables stratification of new products and the consumer change behavior needed for adoption, into four logical categories, stratified into the four quadrants as shown below:
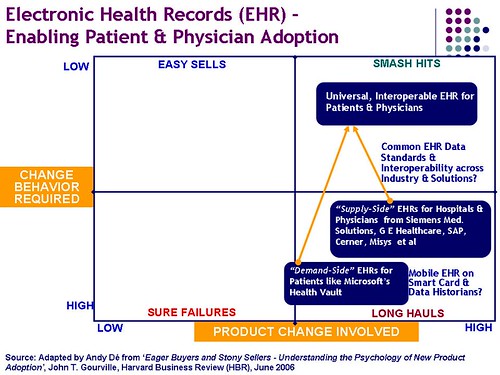
* Low Product Change (“me-too†products) with Significant Change in Customer Behavior needed, usually is a recipe for disaster (“Sure Failureâ€), and is manifested in the 70% of new products and services that fail within a year of introduction or less.
* Low Product Change demanding little change in Customer Behavior (product line extensions of a very successful category like the iPod for instance) is classified as an “Easy Sellâ€, and primarily involves market and channel awareness to drive sales.
* High Product Change (significantly enhanced perceived value from a new category, for instance) with a Significant Change in Customer Behavior will call for a “Long Haul†and slow, phased user adoption based on psychographic and benefit segmentation (early adopters and innovators acting as references for the mainstream market). PHRs and EHRs and products like the Segway can be currently estimated to be positioned here.
* High Product Change (significantly enhanced perceived value) that demands little change in Customer Behavior is usually the recipe for a “Smash Hitâ€, since the compelling value proposition without significant learning curve effects, is sufficient for the customer to adopt. Apple’s new iPhone is an exemplar in this category.
Using this framework as the blueprint for EHR adoption, I have mapped PHRs and EHRs below as “Long Hauls†that will demand significant efforts from the vendors to enable large scale customer adoption to turn these into “Smash Hits“ as shown above. One can argue that legislation and regulations demanding EHR adoption in hospitals across the country, and availability of patient records in electronic format using outsourced transcription services etc. will ensure rapid EHR adoption and the more daunting challenge is getting patients to embrace PHRs like Microsoft’s Health Vault.
That is rather simplistic and does not address significant challenges associated with EHR adoption such as common industry data standards, data interoperability across competing solutions, data capture and analysis etc. that need to be solved to ensure large scale adoption, and presents a huge opportunity for healthcare solution vendors like G E Healthcare, Siemens Med. Solutions, SAP, Cerner, Misys etc.
I will choose to focus this blogpost on PHR adoption by patients in this blogpost.
The PHR Product Lifecycle’ and associated challenges – An “Enlightened Prosumer’s” Vision and Prognosis
Personal Health Records (PHRs) can be prognosized to evolve over a four stage “PHR Product Life Cycle†as below, from my “prosumer vision and perspective†with their associated challenges that will need to be addressed, to ensure significant customer adoption, as below:Â
1. Personal Health Record (PHR) with Healthcare Search– a repository of patient records searchable by keyword, date and therapeutic area that can be shared with physicians and hospitals on demand i.e. the current state, exemplified by the Microsoft Health Vault Platform. The typical records Microsoft envisions being stored in the Health Vault range from fitness-related activities to basic measurements, such as blood glucose and blood pressure, discharge summaries from hospitalizations, lab results, medications and health history.
The single largest challenge today is to enable patients to collect, scan, upload, store and share electronic copies of their paper data that is currently stored in the manila folders in their physician’s offices, which is not trivial, by any stretch of the imagination. While tech-savvy “enlightened prosumers†are sold on the benefits of anytime, anywhere access and can easily scan and upload copies of their medical records, or leverage utilities like Microsoft’s Health Vault Connection Center, to do so, this can be a daunting proposition for the majority of consumers/patients, who are challenged with even mastering their computers, cameras and cell phones.
It is this author’s prognosis that there is an “Adoption Paradox” that will significantly impede customer adoption of the Demand-Side or Personal Health Records (PHRs). Most healthy patients have little incentive to create a PHR to be able to access their records on demand, anytime, anywhere. The PHR presents the most compelling value proposition as a life saving tool for patients with acute or chronic conditions who are vulnerable to sudden, unforeseen attacks that could potentially be fatal. Unfortunately, most of these patients (the prime target segment for the PHR) are also the least likely to have the technical expertise, resources or penchant for creating their PHR and putting it online, given the complexity involved.
There are at least three ways to alleviate this burden. First, provision of a scanning, and upload service ideally at a physician’s office that may demand a shared investment in the hardware and software from the EHR vendor and the hospital. This is far easier at hospitals that have already adopted supply-side EHR that usually provide PDF documents as standard outputs. Secondly, creation of a credit card sized USB based hardware device that would serve as a data capture, storage and retrieval device i.e. the mobile PHR that the patient can carry anywhere and access on any PC worldwide. Uploading the documents in PDF, word or graphic formats at the physicians office and automatic upload on linking with a broadband Internet connected PC via the USB ports at home, would go a long way towards enabling adoption. The third and most obvious, yet challenging mechanism is for patients to obtain electronic or hand written copies of their records and scan or enter them into the PHR at home at their convenience, leveraging utilities such as those provided by Microsoft(Health Vault Connection Center) above. Easing the burden of data entry, paper record scanning and upload is perhaps the single largest barrier to patient adoption that Demand-Side EHR or PHR vendors will have to transcend.
Linking content pertaining to cardiac disease management or diabetes from providers like WebMD, as well as embedded search algorithms (like Microsoft’s Health Vault Search) enables prosumers and patients to educate themselves on the latest research and their associated therapeutic outcomes and also lower their search costs on finding the best possible treatment from an array of branded, and reputed companies like Johnson & Johnson, Novartis, Pfizer, Medtronic, St. Jude Medical, Boston Scientific, Amgen, Genentech or the Mayo Clinic as examples.
Another real design consideration is the potential dissonance from Physicians and Hospitals since availability of PHRs would lower the cost of switching providers for patients and also provide hitherto impossible transparency into the costs of treatment. However, given the current regulations to drive mandatory adoption of EHRs across hospitals, this is the “new reality†that providers (physicians and hospitals) would need to reconcile themselves to and tradeoff against the significantly improved efficiency, cost-effectiveness and patient empowerment and satisfaction.
This would assure significant value to patients in terms of anytime, anywhere access to their critical healthcare information, the ability to share this information with physicians, relatives and hospitals on demand, and also lower their search costs on finding the best possible health alternatives.
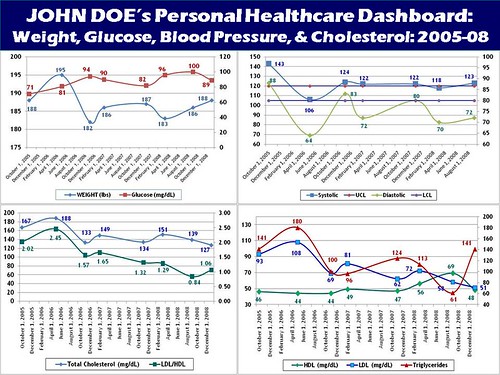
 2. Personal Health Dashboard and Health Commerce – is the next stage in this evolution of the PHR, aimed at providing a single unified overview of a patient’s health, lower search costs, as well as enable online commerce to re-fill prescriptions, order home devices, and schedule physician and service provider appointments (in an ideal world).
 Given the sophistication of currently available portal technologies like Microsoft’s Sharepoint and SAP’s NetWeaver to name a few, delivering a rapidly configurable personal health dashboard, targeted at tech-savvy early adopters and innovators is highly desirable. Having a single dashboard display the results of my last annual check up, my vital signs including height, weight, blood pressure, sugar and cholesterol levels, hyperlinked to their associated medical records, physicians, and potentially content research resources (like WebMD, for instance) would be extremely useful- here is a mock up version of a personal health dashboard crafted by this author as an illustrative example.
 Additional desirable benefits would be electronic reminders (both online as well as text messages sent to cell phones or PDAs) to re-order prescriptions from mail order providers, as well as the ability to schedule appointments for annual check ups with a general practitioner or with specialists as needed. Integration of the PHR with the supply side EHRs and content from insurance providers like Aetna, would also enable access to the transactions associated with each physician visit or cost of medications, to track healthcare expenses accurately.
 Over time, with evolution of common data interoperability standards, it is not inconceivable for supply side EHRs from hospitals to be integrated with the demand–side (personal) EHRs as shown in the adoption blueprint above, that will further accelerate both patient and physician adoption.
 This would enable fairly painless data transfer from the hospital/ physician’s EHR to the patient’s PHR and also provide transparency into the costs associated with treatment, procedures and medication that is a huge challenge today.
 Key anticipated benefits to patients would be a single unified view of their critical vital signs, superior compliance with needed diagnosis and medication, higher transaction efficiency, as well as higher transparency into the procedures and associated costs.
3. Dynamic Personal Health Historian with Exception based Management is the logical next step in the evolution of the demand side PHR. Given the huge numbers of perhaps the most prosperous retirees in the history of North America who will demand proactive intervention based healthcare (as envisioned in my previous blogpost – Can Life Sciences and Healthcare enable my evolution from “Passive Patient†to “Enlightened Prosumerâ€?), the PHR will need to evolve into a Personal Health Historian. This will demand that diabetes monitoring meters from J&J’s Life Scan division, or implanted medical devices like pacemakers and defibrillators from Medtronic, St. Jude Medical and Boston Scientific can interact with and upload streams of vital sign data (blood pressure, sugar levels, pulse rates, electrical impulses etc.) into both demand and supply side EHRs, wirelessly (leveraging blue tooth, RFID or wireless telemetry) to enable proactive intervention when these vital signs are in violation of physician determined threshold levels.
While this is a daunting challenge, this problem of a far greater complexity has already been well addressed in a manufacturing environment. Data Historians from companies like Invensys Wonderware, G E Fanuc and Siemens Automation capture very large amounts of data at a milli-second frequency from manufacturing equipment on the plant floor and also enable data retrieval, analysis and exception based management. Companies like G E Healthcare and Siemens Medical Solutions can be anticipated to borrow these currently available technologies from their sister organizations to render them viable in a supply side EHR context. The challenge then for a demand side EHR solution like Microsoft’s Health Vault is to capture these data streams and appropriately store them for retrieval, analysis and exception management for the patient. This can potentially be accomplished thru the mobile PHR/EHR solution referred to above, with blue tooth, RFID or wireless telemetry capabilities. As well, ability to interact with this mobile PHR/EHR need to be built into the next generation of devices from companies like Life Scan, Medtronic, St. Jude Medical, Boston Scientific etc., as well as the next generation of home based monitoring devices like blood pressure monitors.
For instance, sugar levels in diabetic children being monitored by a Life Scan device could be transmitted to the PHR. Violation of physician prescribed threshold levels, could trigger alerts to parents and the physician, ensuring rapid intervention to preclude further exacerbation. A similar paradigm can be envisioned for middle aged and senior patients with wearable or implanted devices, triggering off compliance reminders or proactive intervention before a serious life impacting event takes place, that would serve to both enhance their span and quality of life as well as lower costs of treatment, by minimizing emergencies, as laid out in my previous blog-post (Can Life Sciences and Healthcare enable my evolution from “Passive Patient†to “Enlightened Prosumer�)
 As well, bidirectional propagation of data on unforeseen outcomes in patients, transmitted to Pharma or Medical Devices manufacturers in near time would alert them on the adverse event implications of their products and enable them to address this within their innovation life cycle, to minimize the unforeseen and undesirable patient and financial impact of their new products. This is distant reality but definitely within the realm of possibilities.
 There are significant benefits that can be delivered to patients using an exception based management approach to personal healthcare as suggested above. These include a higher quality and span of life thru superior therapeutic outcomes delivered at a lower cost per patient.
4. The Personal Healthcare Expert System is perhaps the “Holy Grail of Personal Healthcare†that PHRs should aspire to evolve into. This would involve incorporation of state-of-the art heuristics, neural networks, learning agents, decision support and predictive analytics based technologies that would be integrated with the Personal Health Historians from the previous stage.
 In this paradigm, healthcare data would not only be stored but also analyzed against patient history and benchmark data from similar patient populations. Learning agents would assimilate patient history, behavior and responses to previous treatment to prognosize potential events well before they happen. This would alert patients and point them for diagnostic check ups from qualified physicians, with data on allergies, adverse reactions to medication types etc. to ensure a superior therapeutic outcome pre-empting and precluding incidence of debilitating events like cardiac or diabetic attacks or strokes, the largest causes of deaths in North America today.
 The impact of these personal healthcare systems would be significant in terms of significant life impacting events avoided for the most “at-risk†patient population as well as the huge reduction in treatment costs that would result from their adoption. As well, this would potentially free physicians from mundane checkups and free up time to devote to critical patients as well as keep up with the latest research to better equip them to deliver the best possible outcomes for their patients.
 Significant benefits for patients and providers from deployment of such systems would include reduction of life threatening events (and risks thereof) and associated costs for patients especially, the “at-risk patient population”, as well as the Total Cost of Healthcare (TCH) per patient per treatment, which would significantly contribute to making healthcare more affordable in North America.
This is my humble attempt at visioning the product life cycle that demand-side EHRs or Personal Health Records (PHRs) can be anticipated to evolve thru, to enable widespread patient adoption and also meet the needs of the “enlightened prosumers†that “passive patients†are transforming into.
It will indeed be fascinating to observe and map the trajectory that Microsoft’s Health Vault Platform for PHRs and competing solutions move thru, to enable customer adoption, against this “outside-in blueprint” and more importantly, the impact of this adoption on quality and cost of patient treatment. As always, your comments, feedback and perspectives are welcome.
 Go Home
Go Home
Comment on 7.16.2010
Congratulations on being quoted in the Washington Post! I read your blogposts regularly and find them thought provoking, visionary and insightful – good job!
-Rich Coutinho
Comment on 4.20.2011
Good for you! I also plan to create my own personal health record. Just curious about it. Anyway, I enjoyed reading your post. Thanks for sharing. -mel-